Value-based Health
New Value-based Payment Models at UNC Health
Value-based healthcare has been put forth as part of the solution for America’s growing healthcare cost problem. Slowly, it is arriving. Fee-for-service (FFS) payment-based models, still the most common, are based on the notion that more care = better care. While partly true (e.g. primary care patient engagement), it also leads to misaligned incentives and contributes to decoupling care from clinical outcomes; for example, endoscopy for treatment of GERD (Shaheen et al. 2012).
This week we learned about UNC’s adoption of a Next Generation Accountable Care Organization (ACO) model, called UNC Senior Alliance. Launched in 2017, it is based upon a model developed at CMS’s Innovation Center and intends to test financial incentives for Medicare beneficiaries, that is, cost effective care / shared savings model. In other words, maintain key quality measures and decrease costs - you keep the difference. It should be noted that this only applies to Medicare reimbursement and particularly relevant for UNC Health given the significant proportion of Medicare beneficiaries it serves.
Here is a summary of Quality results from 2018 that shows the associated measures. It seems headed in the right direction although data is limited and not current. In 2018 UNC reported a net savings of $65,885, up from a loss in 2017 of $2.5M. Progress but we’re interested to see if the trend holds for 2019-2020.
The Next Generation ACO model nationally is a bit more uncertain, see below for the latest takeaway on the program (summary PDF):
“During its first two years of performance, the NGACO model was associated with a $123.2 million reduction in Medicare Parts A and B spending (down 0.6%, p<.05), but a $93 million increase in net Medicare spending (up 0.4%, not significant). In the 2017 performance year, the model was associated with insignificant gross spending reductions and a significant net loss to Medicare ($115.6 million spending increase, up 0.7%, p<.05). Reductions in post-acute care spending contributed to a modest decline in gross Medicare spending, but this savings was offset by the shared savings disbursement. The model did not show a discernible impact on quality of care. Planned changes to the model’s financial methodology in Performance Years 4 and 5 (2019 and 2020) are expected to alter shared savings payments in those years and affect estimates of net impact when those years are evaluated.”
Healthcare spending and specifically gross Medicare spending has many inputs, some of which are addressed with the new model. Culture changes with an organization, changes to medical billing and clinical practice will ultimately drive change - more time is needed clearly to realize full potential. I’ll be interested to monitor updates on this, and other models nationally.

Mixed results across cohorts How does this impact innovation and Medtech? Value is fundamental in business; however how exactly that’s implemented on the healthcare reimbursement and payment end has always been murky, particularly early in the innovation process. A cheaper product and with clearly understood positive clinical outcomes is a good bet, but that’s rarely known without significant clinical research investment. Our value model at FastTraCS incorporates four interrelated components: (1) cost of care, (2) clinical outcomes, (3) patient access to care and (4) provider satisfaction. As results are reported on this, and other value-based payment models, we’ll continue to reassess the relative weighting for each component. Cost disruptive solutions may have an even better chance of success compared to historical FFS-based payment models.
Payment models which incorporate financial incentives, emulating a free market, enable a clearer sense of viable business models and innovation strategies. If you can offer an overall cheaper solution while maintaining quality, adoption incentives are more straight-forward. The hope is that such models offer a sliver of certainty among a sphere of other commercial uncertainty. The landscape is constantly in flux: marketed products, population health, clinical guidelines, patentable whitespace, comparative effectiveness outcomes and financial markets can all pull the lever on success or failure.
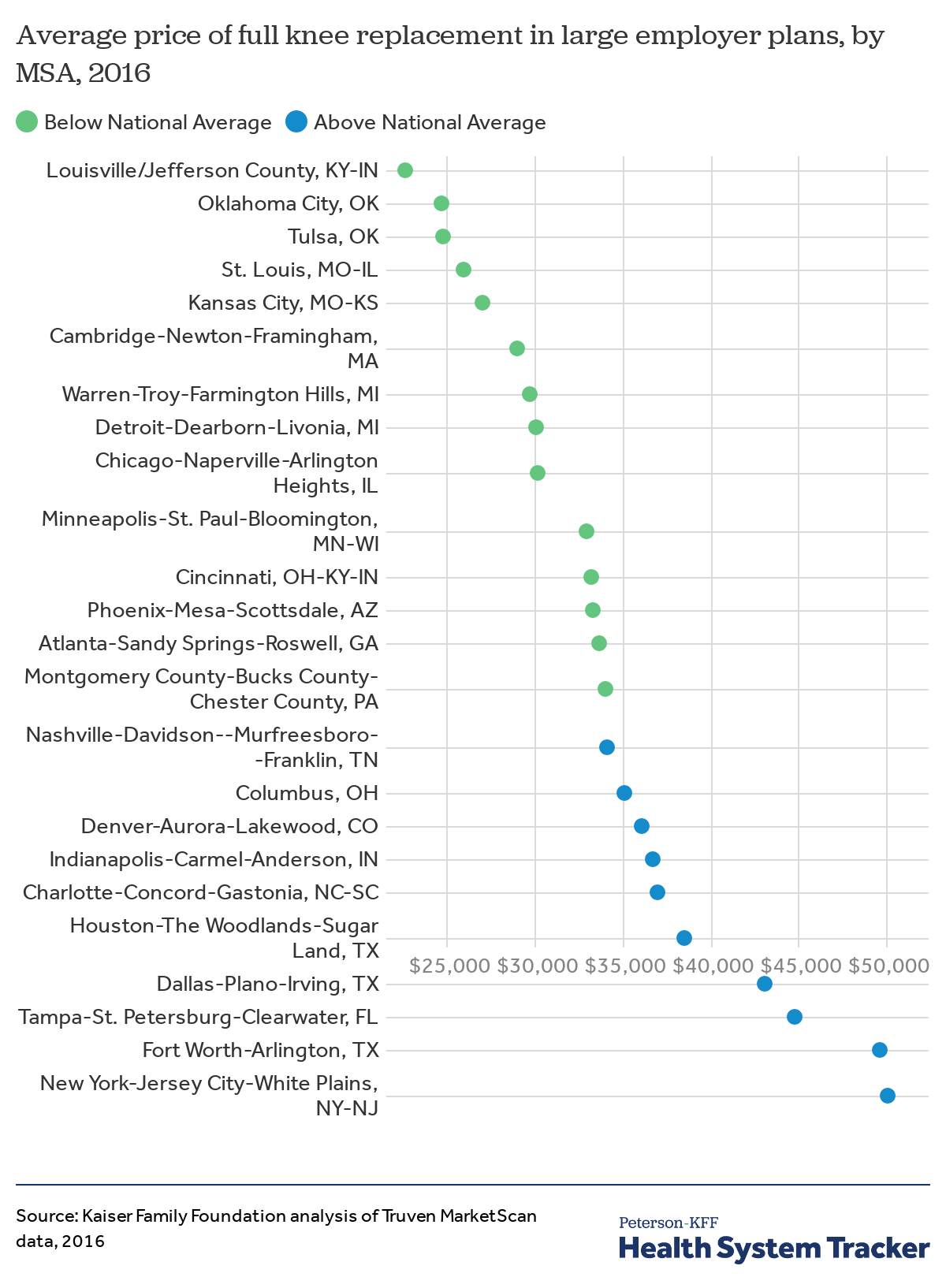
One final note, I highly recommend listening to a podcast featuring surgeon and author Marty Makary, MD, MPH (Peter Attia’s Drive Podcast w/ Marty). Marty is a Professor of Surgery at Johns Hopkins and my new favorite advocate on this topic. He outlines specific systemic challenges to healthcare spending, backed up with data and significant personal experience. I found the discussion about Pharmacy Benefit Managers (PBMs), hospital contracts and price ranges for MRIs (another example for knee replacements) all extremely interesting. He’s published a book on the topic called The Price We Pay which was published last year. Here is his clinical background for those interested.
{kind=link}
References
Shaheen, Nicholas J, David S Weinberg, Thomas D Denberg, Roger Chou, Amir Qaseem, Paul Shekelle, and Clinical Guidelines Committee of the American College of Physicians. 2012. “Upper Endoscopy for Gastroesophageal Reflux Disease: Best Practice Advice from the Clinical Guidelines Committee of the American College of Physicians.” Ann. Intern. Med. 157 (11): 808–16. https://doi.org/10.7326/0003-4819-157-11-201212040-00008.