Forecasting Market Potential using Diffusion of Innovations Theory
The launch of a new product is risky. Sure, you’ve talked with customers, solicited opinions from consultants and done your market research, but how confident can one be prior to actually selling it?
One theory, called Diffusion of Innovations, tries to tackle the age old challenge
Will the dogs eat the dog food?

Diffusion of Innovations Theory
The Diffusion of Innovations theory, developed by sociologist Everett Rogers in 1962, was an influential set of ideas in understanding how new products and technologies gain momentum and spread through different populations (Rogers, Singhal, and Quinlan 2014). This approach is technology-agnostic, though has been applied to pharmaceuticals, MedTech and other industries.
At its core, the theory describes how an innovation interacts over time within a social system, and the importance of branding and organic marketing (e.g., word of mouth).
Key Elements of Diffusion
There are five key elements are:
| Element | Definition |
|---|---|
| Innovation | Innovation as a broad category, relative to the current state-of-the-art. Any idea, practice, or thing that is perceived as new by an individual. |
| Adopters | Adopters are individuals, but can also be organizations (businesses, schools, hospitals, etc.), clusters within social networks, or countries. They include innovators, early adopters, early majority, late majority, and laggards.- |
| Communication channels | Diffusion takes place among groups of people. And communication channels allow the transfer, or diffusion, through the social network. |
| Time | Time is essential to allow for new ideas, practices or things to be adopted. |
| Social system | The social system is conduit through which ideas move. These could be organizations, professional groups, social media or communities. |
Qualities of Innovation
In his book, Rogers outlined five qualities that people use to decide if they buy a product:
- Relative Advantage: The extent to which an innovation is perceived as better than the option it replaces, influencing how quickly it is adopted.
- Trialability: The ease with which an innovation can be tested on a limited basis, reducing the perceived risk of adoption.
- Observable Results: The visibility of the benefits of an innovation, which can encourage wider adoption through social proof.
- Compatibility: The degree to which an innovation aligns with the existing values, past experiences, and needs of potential adopters, affecting its integration into societal norms.
- Simplicity/Ease of Use: How easy and user-friendly the innovation is, determining the speed and extent of its adoption by minimizing the effort required to learn and implement.
These qualities strongly influence product adoption, though other more healthcare specific qualities are:
- Hospital Infrastructure Support: The ability of current hospital systems to incorporate new innovations without significant investment or change, crucial in healthcare technology adoption.
- Workforce Skill Enhancement: The extent to which an innovation requires new skills and how it impacts the performance and satisfaction of the workforce.
- Reimbursement: The financial model associated with an innovation, particularly how it impacts the cost and payment structures within its field of use.
- Quantifiable Economic Benefit: The clear, measurable economic advantages provided by an innovation, often a decisive factor in its adoption.
- Workflow Enhancement: The degree to which an innovation improves or integrates into existing workflows, improving efficiency and effectiveness.
By evaluating these, we can develop a forecasting method to design and implement new products. For example, we may recruit survey participants to rate each one on a 5-point scale.
With data in hand, we use decision-making criteria (e.g., high adoption > 4.2) to estimate the likelihood of product success and moreover, achieving critical mass, a tipping point during Early Majority adoption that leads to self-sustaining growth.
Bass Diffusion Model
The Bass model or Bass diffusion model was developed by Frank Bass (Bass 1969), building on the work of Everett Rodgers. Frank Bass’s contribution included a differential equation that models sales over time, using two coefficients (i.e., p coefficient of innovation, q coefficient of imitation). This model is commonly used marketing.

Forecasting Adoption of Statins using Bass
The use of the Bass Model equation for new medications, specifically statins, has been shown to realistically model adoption and diffusion (Dunn et al. 2012). The team evaluated how quickly statins are adopted by healthcare providers and patients, factoring in perceived innovation (hot news of statins) and imitation (how peer influence accelerates their use). Other groups have applied this approach to patent roadmapping (Jeong et al. 2015), public health (Iqbal and Zahidie 2022), branded/generic drugs (Landsman, Verniers, and Stremersch 2014) and COVID-19 (Eryarsoy et al. 2021).

Prototyping
Let’s create some dummy survey data and see how this might work.
Similar to other innovation frameworks like I-Corps or Biodesign, identifying and surveying appropriate stakeholders will lead to insights; however, insights are often anecdotal and not generalizable. This alone lowers confidence in decision-makers when evaluating a Go/No-Go. Though using a more quantitative approach, like Diffusion of innovations or Jobs-To-Be-Done, teams can augment qualitative data and create stronger, more powerful arguments for product development.
Here is an example of a survey question:
Based on your understanding of this product, on a scale of 1 - 5, rate the relative advantage versus the current product in use.
VivSustain
Let’s start with a hypothetical product, VivSustain.
VivSustain, an Intelligent Antiretroviral Therapy Implant, simplifies HIV management by ensuring continuous dosing of antiretroviral drug delivery. Designed for those who find it hard to manage daily medication, VivSustain offers a discreet, maintenance-free 12-month implantable therapy that maintains optimal viral suppression and combats drug resistance.
Say we survey 100 stakeholders, across adopter segments (i.e., innovators, early-adopters, etc), then we ask them to rate our 10 Diffusion of innovations qualities on a scale of 1-5, 5 being the best. Here is my python code to generate the data:
import numpy as np
import pandas as pd
# Define means and standard deviations for each quality
means_sd = {
"Relative Advantage": (3.6, 0.8),
"Trialability": (4.2, 1.2),
"Observable Results": (4.3, 0.5),
"Compatibility": (3.5, 1.3),
"Simplicity/Ease of Use": (4.5, 0.4),
"Hospital Infrastructure Support": (3, 2),
"Workforce Skill Enhancement": (2, 2.2),
"Reimbursement": (3.9, 0.8),
"Quantifiable Economic Benefit": (2.7, 0.8),
"Workflow Enhancement": (3, 2.4)
}
# Define ranges for each quality
ranges = {
"Relative Advantage": (2, 5),
"Trialability": (2, 5),
"Observable Results": (3, 5),
"Compatibility": (1, 5),
"Simplicity/Ease of Use": (3.5, 5),
"Hospital Infrastructure Support": (1, 5),
"Workforce Skill Enhancement": (1, 4),
"Reimbursement": (2, 4),
"Quantifiable Economic Benefit": (1, 4),
"Workflow Enhancement": (1, 4.2),
}
num_respondents = 100
# Generate survey data with specified means and SDs
survey_data = {}
for key, (mean, sd) in means_sd.items():
low, high = ranges[key]
data = np.random.normal(mean, sd, num_respondents)
# Truncate values to stay within specified ranges
data_clipped = np.clip(data, low, high)
survey_data[key] = data_clipped
# Transform to data frame
survey_df = pd.DataFrame(survey_data)
# Round to the nearest whole number
survey_df = survey_df.round()
# Save file to csv
survey_df.to_csv("vivsustain_survey_results.csv", index=False)
Survey Data Results
Relative Advantage | Trialability | Observable Results | Compatibility | Simplicity/Ease of Use | Hospital Infrastructure Support | Workforce Skill Enhancement | Reimbursement | Quantifiable Economic Benefit | Workflow Enhancement |
|---|---|---|---|---|---|---|---|---|---|
5 | 4 | 4 | 4 | 5 | 5 | 2 | 3 | 3 | 1 |
3 | 2 | 4 | 3 | 5 | 1 | 1 | 4 | 2 | 4 |
4 | 3 | 4 | 3 | 5 | 3 | 4 | 4 | 3 | 1 |
Figure 1 presents a heat map based on the *hypothetical* survey data, showing the rating frequency across our ten qualities. Intense blue reflects a high frequency of responses.
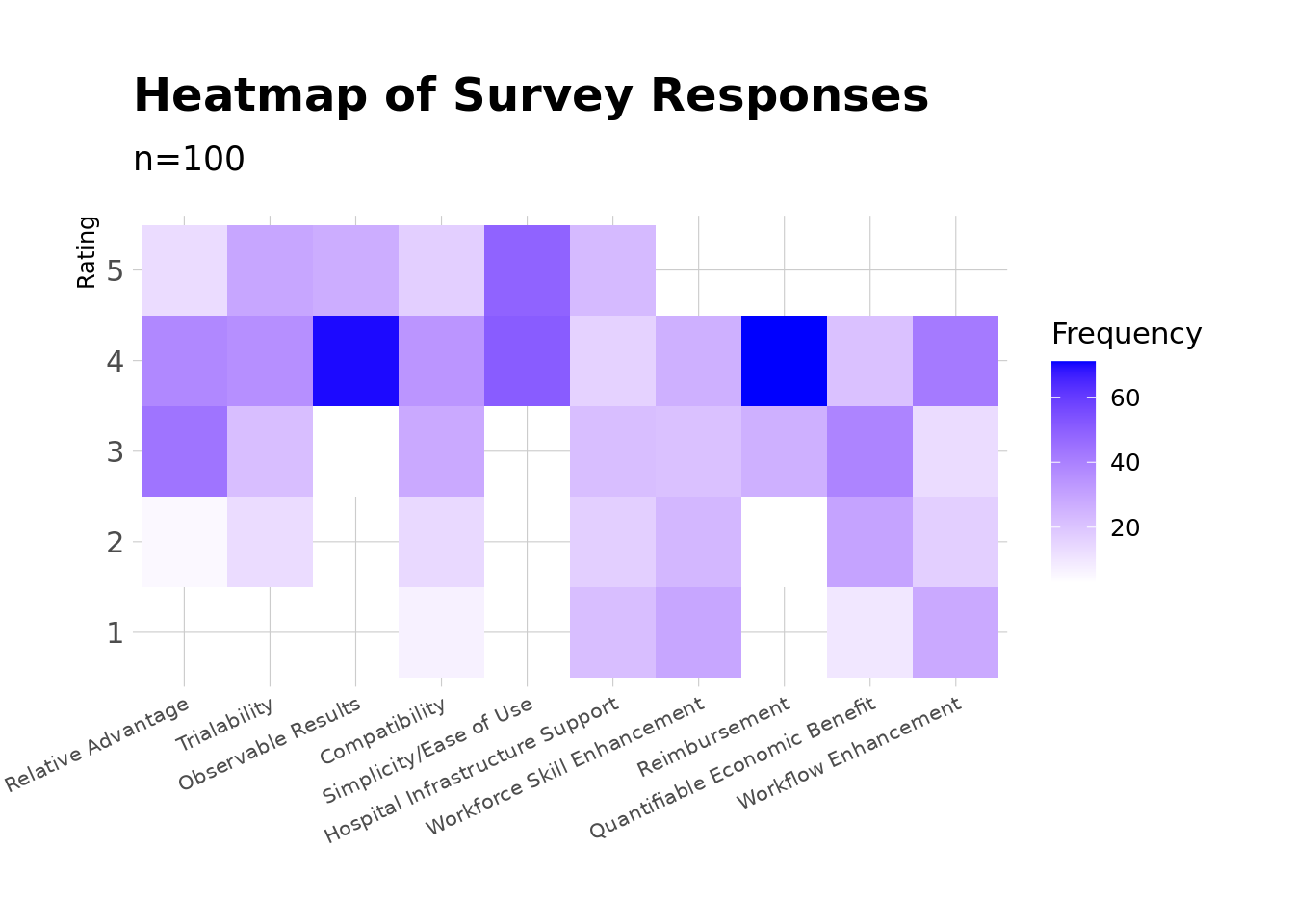
Figure 1: VivSustain Survey Heatmap
The results represent a generally favorable view of the product. In other areas there is uncertainty. Trialability, Simplicity/Ease of Use, and Reimbursement were highly rated (as shown in blue). These areas suggest the product is user-friendly, feasible to test clinically and has a favorable reimbursement path. Observable Results also was rated highly, suggesting that the product’s value is apparent people.
Workforce Skill Enhancement and Quantifiable Economic Benefit show a significant spread of lower ratings, signaling concerns about cost-effectiveness and training burden. Mixed responses for Compatibility, Hospital Infrastructure Support, and Workflow Enhancement reflect more ambiguity.
Conclusion
Wrapping up, our exploration of the Diffusion of Innovation framework applied to the hypothetical product, VivSustain, underscores the inherent uncertainties of any new product launch. It’s an asymptotic endeavor towards certainty, one that is never fully realized. For any innovation, the ultimate aim is to ascertain the likelihood of market adoption—whether “the dogs will indeed eat the new dog food,” so to speak.
Medical products typically undergo a lengthy lifecycle and time-to-market. Given the substantial investment required before generating revenue, approaches like the Diffusion of Innovation framework, or other semi-quantitative methods, show promise. If a prospective innovation scores low on key qualities, it would be prudent to consider reassessing or even terminating the project early on.
References
Bass, Frank M. 1969. “A New Product Growth for Model Consumer Durables.” Management Science 15 (5): 215–27. https://doi.org/10.1287/mnsc.15.5.215.
Dunn, Adam G, Jeffrey Braithwaite, Blanca Gallego, Richard O Day, William Runciman, and Enrico Coiera. 2012. “Nation-Scale Adoption of New Medicines by Doctors: An Application of the Bass Diffusion Model.” BMC Health Serv. Res. 12 (1).
Eryarsoy, Enes, Dursun Delen, Behrooz Davazdahemami, and Kazim Topuz. 2021. “A Novel Diffusion-Based Model for Estimating Cases, and Fatalities in Epidemics: The Case of COVID-19.” Journal of Business Research 124: 163–78.
Iqbal, Meesha, and Aysha Zahidie. 2022. “Diffusion of Innovations: A Guiding Framework for Public Health.” Scandinavian Journal of Public Health 50 (5): 533–37.
Jeong, Yujin, Keeeun Lee, Byungun Yoon, and Rob Phaal. 2015. “Development of a Patent Roadmap Through the Generative Topographic Mapping and Bass Diffusion Model.” Journal of Engineering and Technology Management 38: 53–70.
Landsman, Vardit, Isabel Verniers, and Stefan Stremersch. 2014. “The Successful Launch and Diffusion of New Therapies.” Innovation and Marketing in the Pharmaceutical Industry: Emerging Practices, Research, and Policies, 189–223.
Rogers, Everett M, Arvind Singhal, and Margaret M Quinlan. 2014. “Diffusion of Innovations.” In An Integrated Approach to Communication Theory and Research, 432–48. Routledge.